Presentation and Mechanisms of Labor
Authors
INTRODUCTION
The fetus undergoes a series of changes in position, attitude, and presentation during labor. This process is essential for the accomplishment of a vaginal delivery. The presence of a fetal malpresentation or an abnormality of the maternal pelvis can significantly impede the likelihood of a vaginal delivery. The contractile aspect of the uterus is another essential aspect of this process. This combination of factors has been classically described as the passenger (the fetus), the passage (the maternal pelvis) and the powers (the uterine contractions). This chapter addresses the impact of the fetus and the maternal pelvis on the labor process.
THE FETUS
To assess the potential impact of the fetus on the characteristics of the labor process, it is important that the obstetrician be knowledgeable of the basic concepts used routinely to describe how the body of the fetus is located in the uterus. The obstetrician should be able to determine the fetal lie, presentation, and position, using the maternal vertebral column and pelvis as reference points, by Leopold's maneuvers, vaginal examination, and if necessary, ultrasound.
Leopold's Maneuvers
Leopold's maneuvers1 consist of an abdominal examination divided into four steps of palpation of the gravid uterus and fetus (Fig. 1). The examiner may be able to palpate the presenting part. In addition, a clinical estimate of the degree of engagement of the presenting part could be made, although the final determination of engagement must be made by way of a vaginal examination. Through use of Leopold's maneuvers, a clinical estimate of the fetal weight also can be obtained, although this is not a formal part of this examination. The accuracy of Leopold's maneuvers can be hampered by the maternal body habitus, the presence of uterine fibroids, multiple gestations, or polyhydramnios. What follows is a description of these maneuvers:
|
Maneuver I: The uterine contour is outlined. The fundus is palpated with the fingertips of both hands facing toward the maternal xiphoid cartilage. This should allow the identification of the fetal parts in the upper pole (fundus) of the uterus.
Maneuver II: Once an assessment is made of the fetal part present in the uterine fundus, the hands are placed at either side of the maternal abdomen. With this maneuver, the examiner will be able to determine the location of the fetal back.
Maneuver III: Using one hand, the examiner will grasp the presenting part between the thumb and fingers. This is done on the lower abdomen, a few centimeters above the symphysis pubis. This will allow the examiner to develop a further identification of the presenting part and assessment of its engagement.
Maneuver IV: This last maneuver resembles the first one, but instead of facing the fundus, the examiner faces the pelvis of the patient. The palms of both hands are placed on either side of the lower maternal abdomen, with the fingertips facing toward the pelvic inlet. This maneuver should allow the identification of the fetal parts in the lower pole of the uterus.
After the abdominal examination, a digital vaginal examination is performed. The status of the amniotic membranes and the degree of engagement of the presenting part are indicators of fetal presentation and position. The vaginal examination also allows the clinician to assess the degree of cervical dilation and effacement. If the presenting part is not easily palpable, it is important that further assessment be obtained by performing an ultrasound examination. The ultrasound should be 100% accurate in diagnosing the type of fetal presentation.
Fetal Lie
Using the techniques described above, the clinician should be able to develop an assessment of the relationship between the fetal and maternal dorsal columns (the longitudinal axis of the human body). If the fetus and maternal column are parallel (on the same long axis), the lie is termed vertical or longitudinal lie. This is the most common lie of fetuses in labor. Contrary to this is the transverse lie, in which the fetus is positioned 90° with respect to the mother's dorsal column. There are variants of these two lies, in which the fetus may be in transition from a vertical to a transverse lie. These are the oblique lies.
A fetus can be in an unstable or variable lie when the head is completely unengaged and floating. This situation is seen mostly in cases of severe polyhydramnios and prematurity. The obstetrician should be aware that a fetus in this particular type of lie is susceptible to a cord accident if the patient is in active labor and her cervix is dilating.
Attitude
In addition to having a lie, the fetus has an attitude. This is defined as the relation of the various parts of the fetus to each other. In the normal attitude, the fetus is in universal flexion. The anatomic explanation for this posture is that it enables the fetus to occupy the least amount of space in the intrauterine cavity. The fetal attitude is extremely difficult, if not impossible, to assess without the help of an ultrasound examination.
Presentation
After the lie of the fetus is assessed, the clinician has to detail the fetus further by describing the lowermost structure of the fetus in the maternal pelvis. This is referred to as the fetal presentation. In a vertical (or longitudinal) lie, the fetal presentation can be either cephalic or breech. In the transverse lie, the presentation is usually the back or shoulder; in the oblique lie, it is usually the shoulder or the arm.
The cephalic presentation can be further categorized based on the degree of flexion of the fetal head: A well-flexed head is described as a vertex presentation, an incomplete flexion as a sinciput presentation, a partially extended (deflexed) head as a brow presentation, and a complete extension of the head as a face presentation.
Breech presentation can be categorized on the basis of the attitude or flexion of the hip and knee joints. If there is flexion at the hip and extension at the knees, the fetus is a frank breech. If there is flexion at both the hip and knee joints, the fetus is a full or complete breech. A footling breech has one or both hips and knees in a partial or intermediate extension; this fetus is sometimes called an incomplete breech.
Presentations other than cephalic or breech in a singleton pregnancy require an abdominal route of delivery. These presentations are uncommon, occurring in less than 1% to 2% of all deliveries. Abnormal presentations occur more often in cases of multiple gestation, usually affecting the second twin. Depending on the clinical condition, vaginal delivery of a malpresenting second twin is possible.
Position
The next step in the assessment of the fetus consists of determining the position of the presenting part. This is a description of the relation of the presenting part of the fetus to the maternal pelvis.
In the case of a longitudinal lie with a vertex presentation, the occiput of the fetal calvarium is the landmark used to describe the position. When the occiput is facing the maternal pubic symphysis, the position is termed direct occiput anterior. If the occiput is between the ischial spines and the symphysis, it is called either a right or left occiput anterior. If the occiput is located halfway between the promontorium of the sacrum and the symphysis, the position is termed either a left or right occiput transverse. As the occiput approaches the sacrum, it becomes either a right or left occiput posterior. When the occiput is straight down (i.e., facing the sacrum or coccyx), the position is called direct occiput posterior. This method of describing the fetal position can be applied to other presentations by substitution of the vertex for the presenting fetal anatomic landmark. In cases of breech presentation, the fetal sacrum is used for position.
With transverse and oblique lies, the shoulder structures (acromion) can be used for the description of position. The incidence of transverse lie has been reported as 0.3%.2 Fetal malformations can cause these (and other) malpresentations. These two types of lies have been associated with grandparity, contracted maternal pelvis, placenta previa, prematurity, polyhydramnios, and uterine abnormalities such as transverse septum or leiomyomas. A patient in her last month of pregnancy with a fetus in a transverse or oblique lie would require an ultrasound and physical examination for the evaluation of any of the above risk factors. If no contraindications are identified, one possible management alternative would be an external cephalic version. The success of external cephalic version in cases of transverse lie has been reported as high as 83%,3 even when performed intrapartum. If an elective cesarean section is to be performed, it should be scheduled for the last week of the pregnancy, because 83% of transverse lies will spontaneously convert to a vertex presentation before 39 weeks.4 This expectant management has to be individualized. Patients showing signs of early labor or those with cervical dilation are candidates for an attempt of external version or delivery by cesarean section before 39 weeks.
The fetal anatomic landmarks used to describe the position in the brow and face presentations are the bregma and the mentum. The outlook of the persistent brow presentation for vaginal delivery is poor. Approximately two thirds of brow presentations will convert to vertex or face.2 Fortunately, this is a rare presentation, with an incidence of only 0.05%.5 If the presentation persists as a brow, a cesarean section should be performed. The incidence of face presentation has been quoted as 0.21% of all deliveries.6 In cases of face presentation, a vaginal delivery can be accomplished most frequently with a mentum anterior position, but the mentum posterior position will impede the fifth cardinal movement of labor (extension). Most fetuses in face or mentum posterior position that do deliver vaginally do so after converting during the internal rotation into a mentum anterior or mentum transverse position.
A fetus in a persistent mentum posterior position could be delivered vaginally if it were very premature or the maternal pelvis large. Most frequently, this will not be the case. More than 75% of fetuses at term with mentum posterior position will require delivery by cesarean section because of labor dystocia. This contrasts with a more than 88% success rate of vaginal delivery with the mentum anterior position.7 In view of these data, many clinicians opt to perform a cesarean section for fetuses with a face presentation and a mentum posterior position, without allowing for a trial of labor. Even if vaginal delivery of a mentum anterior presentation is attempted, the diameter of the presenting part may exceed the maternal pelvic capacity. A situation like this also would require an abdominal delivery. Before allowing vaginal delivery of a fetus in a face presentation and a mentum anterior position, the clinician should exclude the possibility of a fetal malformation causing the malpresentation. The brow and face presentation should alert the clinician to the possibility of a congenital fetal anomaly, such as thyromegaly, cystic hygroma, anencephaly, encephalocele, cervical neural tube defects, and teratomas, that could be preventing the flexion of the head. In addition, maternal factors, such as preterm labor, abnormal pelvis, multiple gestation, and a low-lying placenta, have been associated with deflexion of the fetal head. After excluding the possibility of a fetal malformation with the use of a detailed ultrasound examination, the clinician should then exclude the possibility of a contracted maternal pelvis. If on clinical pelvimetry there are any signs of an abnormal pelvis, the clinician should consider obtaining an x-ray or digital pelvimetry.
In addition to the above presentations and fetal positions, there are compound presentations in which one or more extremities of the fetus will present in addition to the vertex or breech. This has been described as “prolapse of an extremity alongside of the presenting part, both entering the pelvic canal simultaneously.”8 The incidence of this type of presentation has been reported to range from 0.15%9 to 0.4%.10 The most frequent is a vertex and hand combination, which accounts for 58% of the cases.9 This is followed in incidence by a vertex, hand, and umbilical cord combination (17%). It is extremely important that the clinician exclude the presence of an umbilical cord prolapse when evaluating a patient with a compound presentation. Risk factors for this type of presentation include contracted maternal pelvis, preterm labor, small for gestational age fetuses, and grandparity. The majority of women whose fetuses have compound presentations can be delivered vaginally. In a series of 131 patients,10 only 2 required a cesarean section. During the course of labor, the extremity will usually slide to the side of the body and the compound presentation will spontaneously convert to a vertex presentation.
Station
In addition to the fetal lie, presentation, and position, the level or station of the presenting part in the maternal pelvis is an important factor in the labor process. For this assessment, the ischial tuberosities of the maternal pelvis are used as the anatomic landmark structures. If the presenting part is above the spines, it is described by the use of negative numbers. If the presenting part is nonpalpable, it is in a floating station; if it is well applied against the cervix, but above the spines, it can range from -1 to -3. There is a significant subjective variation among examiners in the assignment of station. Some consider these numbers to be equivalent to centimeters. Once a presenting part is at the level of the spines, it is considered to be engaged and at 0 station. Below the 0 station, positive numbers are used. If the presenting part is against the pelvic floor, it is at +3 station.
Cardinal Movements of Labor
To accommodate itself to the maternal pelvic dimensions, the fetus must undergo a series of changes in the attitude of its presenting part. This is required for fetal descent through the birth canal. The cardinal movements of labor in a vertex presentation are as follows:
- Engagement: The vertex is engaged when the biparietal diameter is at the level of the pelvic inlet or lower. In clinical practice, this translates into an occiput palpable at 0 station.
- Descent: This cardinal movement will usually happen concomitant with engagement, and is typically documented late in the active phase of the first stage of labor.
- Flexion: As the vertex descends into the maternal pelvis, it will encounter resistance from the maternal pelvic floor muscles. This will cause the flexion of the fetal head onto the thorax.
- Internal rotation: At the moment of engagement and descent of the vertex into the pelvis, the fetus will be in a transverse position. Because of the anatomic configuration of the pubococcygeus and iliococcygeus muscles, the occiput will be forced to rotate to the symphysis pubis. This is the widest area of the pelvic floor that will allow the passage of the fetus.
- Extension: At the moment of the delivery of the fetal head, the combined effects of the uterine contractions and the pelvic floor result in this cardinal movement.
- External rotation: This movement occurs as a consequence of the alignment of the head of the fetus with its spine as the pressure from the maternal pelvis and muscles on the fetal head is alleviated.
- Expulsion: After delivery of the head, the anterior shoulder will descend under the pubic bone. As it is delivered, it will follow the external rotation of the head of the fetus.
It is important for the reader to understand that these are not separate events. They are all closely related, and some will happen simultaneously.
Concomitant to the cardinal movements, there can be significant molding of the presenting part. This complex process can be deeply influenced by a large number of factors. Abnormalities of the shape and size of the presenting part or maternal pelvis can cause problems affecting not only the capacity of the fetus to descend, but also its internal rotation. Most fetuses initiate the cardinal movements in a occiput transverse position. If its internal rotation were to be disrupted, the fetus could present in an occiput posterior position. Internal rotation can be affected by the administration of epidural anesthesia. If the pelvic floor musculature is suddenly relaxed by a strong epidural block, internal rotation could be directed toward the maternal sacrum, rather than toward the symphysis. In addition, the head of the fetus could become asynclitic. This condition occurs when the head is not in the same longitudinal axis as the fetal vertebral column. The gross appearance of an asynclitic head is that of a lateral tilt toward the shoulder. The major problem of asynclitism is that it causes the head to present a larger diameter to the maternal pelvis than what it would otherwise present. This could lead to labor dystocia due to a relative cephalopelvic disproportion.
Additional problems related to the sudden relaxation of the pelvic floor muscles include possible lack of flexion of the presenting part. In a fetus in a vertex lie, this could result in a brow or face presentation.
Other factors that could influence the position of the presenting part include the maternal position during labor, the presence of fetal or uterine anomalies, and the type of maternal pelvis. In Western society, it has been a common practice for women to labor on their back or side. Midwives frequently have their patients labor in positions other than the back or side so that the occiput on posterior position is prevented, although this practice has not been studied objectively.
THE MATERNAL PELVIS AND ITS VARIATIONS
The shape and size of the maternal pelvis has been the subject of significant evaluation and description. Most of current knowledge on this subject originates from the classic contributions of Caldwell, Moloy, and D'Esopo.11,12 The clinical recognition of the different types of pelves is important because of their different capacity, obstetric significance, and resulting prognostic importance.13
The four major types of maternal pelves and their characteristics are outlined as follows:
- Gynecoid (Fig. 2)
![]() Fig. 2. Gynecoid pelvis. A. Inlet view. B. Lateral view. C. Subpubic arch view.
Fig. 2. Gynecoid pelvis. A. Inlet view. B. Lateral view. C. Subpubic arch view.- A spacious and well-rounded posterior segment
- A An inlet with a slightly ovoid or round shape
- A wide, well-rounded forepelvis (anterior segment)
- A sacrosciatic notch of medium size
- An average sacral inclination and curvature
- A wide subpubic arch
- Wide interspinous and intertuberous diameters
- Bones ranging from medium to delicate in structure
Engagement in this type of pelvis occurs most frequently with the fetus in a transverse position, followed in frequency by the anterior and posterior positions.
- A spacious and well-rounded posterior segment
- Android (Fig. 3)
![]() Fig. 3. Android pelvis. A. Inlet view. B. Lateral view. C. Subpubic arch view.
Fig. 3. Android pelvis. A. Inlet view. B. Lateral view. C. Subpubic arch view.- A wedge-shaped inlet
- A narrow retropubic angle (anterior segment)
- A flat, wide posterior segment
- A narrow sacrosciatic notch
- A forward sacral inclination
- A narrow wedge-shaped “Gothic” subpubic arch
- Converging side walls, narrow interspinous and intertuberous diameters
- Bones ranging from medium to heavy in structure
Engagement in this type of pelvis occurs most frequently with the fetus in a transverse position, followed in frequency by the posterior and anterior positions. The clinician should be alerted by this type of pelvis that the possibility of posterior positions exists.
- A wedge-shaped inlet
- Anthropoid (Fig. 4)
![]() Fig. 4. Anthropoid pelvis. A. Inlet view. B. Lateral view. C. Subpubic arch view.
Fig. 4. Anthropoid pelvis. A. Inlet view. B. Lateral view. C. Subpubic arch view.- A long, narrow, oval-shaped inlet
- A long, narrow, well-rounded anterior segment
- A long, narrow posterior segment
- A very wide, shallow sacrosciatic notch
- A long, narrow sacrum with average inclination and curvature
- A slightly narrow subpubic arch
- Straight side walls with below-average interspinous and intertuberous diameters
- Medium to delicate bones
Engagement in this type of pelvis occurs with the fetus in either an anterior or transverse position, but the anterior position appears to be more characteristic.
- A long, narrow, oval-shaped inlet
- Platypelloid (Fig. 5)
![]() Fig. 5. Platypelloid pelvis. A. Inlet view. B. Lateral view. C. Subpubic arch view.
Fig. 5. Platypelloid pelvis. A. Inlet view. B. Lateral view. C. Subpubic arch view.- A transverse, oval-shaped inlet
- A very wide, round retropubic angle
- A very wide, flat posterior segment
- A narrow sacrosciatic notch
- Average sacral inclination
- A very wide subpubic arch
- Straight side walls with very wide interspinous and intertuberous diameters
- Bones ranging from medium to delicate in structure
- A transverse, oval-shaped inlet
Engagement in this type of pelvis will almost always occur with the fetus in a transverse position. Because of the flatness of the shape of this pelvis, the internal rotation of the vertex can be limited, causing a deep transverse arrest.
The most frequently encountered type of pelvis is the gynecoid, followed by the android, anthropoid, and platypelloid. There are at least 10 mixed forms consisting of combinations of the anterior and posterior segments of the pure types of pelves (Fig. 6). In general terms, one could say that the gynecoid and anthropoid pelves are favorable for vaginal delivery, whereas the android and platypelloid are suboptimal. A significant number of patients will fall into intermediate categories (Fig. 7). A clinical assessment of the maternal pelvis (pelvimetry) is performed routinely by clinicians at the first prenatal visit or upon hospital admission to the labor and delivery unit. This concept of clinical pelvimetry should be mastered by all obstetricians. The clinical pelvimetry should be always documented in the prenatal record or admission note to the labor and delivery unit. In a study published in 1940, Caldwell and colleagues12 reported an interesting finding: Of more than 3000 case studies, only 2% involved contracted pelves, one half of which were due to rickets.
|

|
In addition to trying to determine the type of pelvis, the clinician should attempt to assess its diameter. The two diameters most commonly measured are the diagonal conjugate and the bi-ischial. The diagonal conjugate diameter is the measurement from the inferior border of the pubic symphysis to the sacral promontory. It serves as an estimate of the anteroposterior diameter of the pelvic inlet. This diameter should be greater than 11.5 cm. The bi-ischial diameter is the distance between the ischial tuberosities. The expected diameter should be a minimum of 8 cm. In the pelvimetry report, the clinician also should comment on how hollow the sacrum is, as well as the degree of prominence of the sacral promontory. The angle of the pubis is used to classify the type of pelvis. Convergence of the side walls or prominent ischial spines are unfavorable prognostic findings. Any abnormalities noted during clinical pelvimetry should be carefully documented. These abnormalities should be carefully considered while evaluating the course of labor of a patient. Routine assessment of the maternal pelvis by x-ray studies has largely been abandoned, with the exception of fetuses in a breech presentation.
X-Ray Pelvimetry
The most accepted technique of x-ray pelvimetry was first described in 1944 by Colcher and Sussman.14 Earlier techniques were thought to be technically difficult and cumbersome.15 The Colcher-Sussman technique incorporated the following basic principles:
- Simple intersecting diameters of the true pelvis
- Simple positioning of the patient
- A simple ruler for rapid and direct measurements in centimeters.
With this technique, the intersecting diameters of the inlet, midpelvis, and outlet are added to give three respective values. The normal ranges for these values are 22 to 24 cm for the inlet, 20 to 22 cm for the midpelvis, and 16 to 18.5 cm for the outlet. Fig. 8 and Fig. 9 show the positioning of the patient for x-ray pelvimetry.
|

|

Unfortunately, x-ray pelvimetry has fallen short of its expected clinical performance. Several articles have demonstrated its limited role in contemporary obstetric practice.16,17 There are several reasons for this:
- In cases of a vertex presentation, it is clear that a significant incidence of false-positives and -negatives occurs with this technique. Vaginal delivery can be accomplished in cases of borderline adequate pelvimetry. This is secondary to the capacity of the fetal head to mold.
- The technique is unable to assess the impact of the maternal soft tissue of the vaginal walls on the pelvic capacity.
- There is a concern regarding the development of childhood malignancy, specifically leukemia, secondary to fetal exposure to ionizing radiation.18,19
The data on this subject are extremely controversial; however, the relative risk of malignancy appears to be small.
More recently, the use of modern radiographic techniques, such as computerized tomography (CT)20,21,22,23,24,25,26 and magnetic resonance imaging (MRI),27,28,29 have been reported as more reliable tools for pelvimetry examination than flat x-ray films. The use of CT scanning in preference to conventional radiography can be justified on the basis of ease of performance, interpretation, and decreased radiation exposure to the fetus.23 It also is possible to evaluate the fetal lie and position with CT scanning.24
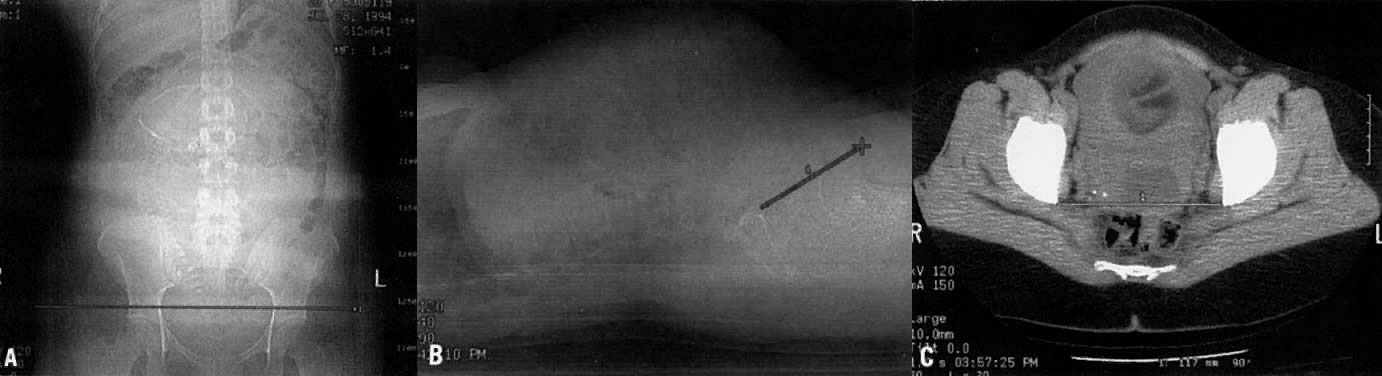
The technique for CT pelvimetry was first described by Federle and co-workers.20 Views are obtained for anteroposterior and lateral projections (Fig. 10). These allow measurement of the transverse and anteroposterior diameters of the pelvic inlet and midpelvis, respectively. The anteroposterior diameter of the inlet should be a minimum of 10 cm. The transverse diameter of the inlet should be a minimum of 11.5 cm. A third view is obtained at the level of the fovea of the femoral heads. This last view is a single axial tomographic section. It is utilized to measure the bi-ischial diameter, which should be a minimum of 9.5 cm.23
|
MRI has these same advantages plus the lack of any ionizing radiation. In addition, it has a higher resolution and contrast than CT.27 MRI is contraindicated in patients with a metal prosthesis. At present, there have been no deleterious effects to the fetus caused by the use of MRI.28
One clear disadvantage of CT and MRI over plain x-ray pelvimetry is their cost: MRI costs nearly $1,000, and a CT study costs between $200 and $300. In contrast, x-ray pelvimetry costs less than $200. It is possible to justify the additional cost of the digital techniques on the basis of their better quality and lower or absent ionizing radiation. To our knowledge, there has been only one comparative study of CT versus x-ray pelvimetry.21 It was a small trial, with only four patients reported. The data suggested that more precise measurements can be obtained with CT pelvimetry. Reported studies on MRI pelvimetry have all been descriptive.
The availability of digital techniques is sometimes limited. Not all institutions have CT or MRI units; for those that do, problems exist because these units must be shared by all clinical services within the institution.
CONCLUSIONS
It is essential for any clinician practicing obstetrics to be familiar with the concepts of fetal lie, attitude, presentation, position, and station. During labor, there will be a series of changes in the position of the presenting part that are needed for the fetus to pass through the maternal pelvis. Knowledge of the type of maternal pelvis is critical for proper monitoring of this process. The different types of maternal pelves will have a significant influence on the course of labor. As mentioned before, fetal or uterine anomalies can cause abnormalities of the fetal lie, presentation, and position. The presence of these problems should prompt the clinician to perform the necessary evaluations to identify the possible etiology of these abnormalities. Increased availability of new modalities in the field of radiology, such as digital radiographic techniques, will provide us with tools for better assessment of fetal malpresentation.
REFERENCES
Leopold S: Die Leitung der regelmässigen Geburten nur durch a¨ussere Untrsuchung (Conduct of normal births through external examination alone). Arch Gynaekol 45: 337, 1894 |
|
Cruikshank DP, White CA: Obstetric malpresentation. Am J Obstet Gynecol 116: 1097, 1973 |
|
Phelan JP, Stine LE, Edwards NB et al: The role of external version in the intrapartum management of the transverse lie presentation. Am J Dis Child 151: 724, 1985 |
|
Phelan JP, Boucher M, Mueller E et al: The nonlaboring transverse lie: A management dilemma. J Reprod Med 31: 184, 1986 |
|
Fields H, Nelson PK: Errors of presentation. Am J Obstet Gynecol 78: 539, 1959 |
|
Cucco UP: Face presentation. Am J Obstet Gynecol 94: 1085, 1966 |
|
Benedetti T, Lowensohn RI, Truscott AM: Face presentation at term. Obstet Gynecol 55: 199, 1980 |
|
Eastman NJ, Hellman LN: Textbook of Obstetrics, 13th ed. New York, Appleton-Century-Crofts, 1966 |
|
Goplerud J, Eastman NJ: Compound presentation: A survey of 65 cases. Obstet Gynecol 1: 59, 1953 |
|
Breen JL, Wiesmeier E: Compound presentation: A survey of 131 patients. Obstet Gynecol 32: 419, 1968 |
|
Caldwell WE, Moloy HC, D'Esopo DA: Further studies on the pelvic architecture. Am J Obstet Gynecol 28: 482, 1934 |
|
Caldwell WE, Moloy HC, D'Esopo DA: The more recent concepts of the pelvic architecture. Am J Obstet Gynecol 40: 558, 1940 |
|
Caldwell WE, Moloy HC: Anatomical variations in the female pelvis and their effect in labor with a suggested classification. Am J Obstet Gynecol 26: 479, 1933 |
|
Colcher AE, Sussman W: A practical technique for Roentgen pelvimetry with a new positioning. Am J Roentgenol 51: 207, 1944 |
|
Moloy HC: A new method of Roentgen pelvimetry. Am J Roentgenol 30: 111, 1933 |
|
Laube DW, Varner MW, Cruickshank DP: A prospective evaluation of x-ray pelvimetry. JAMA 246: 2187, 1981 |
|
Parsons MT, Spellacy WN: Prospective randomized study of x-ray pelvimetry in the primigravida. Obstet Gynecol 66: 76, 1985 |
|
Brent RL: The effects of radiation on embryogenesis. J Reprod Med 12: 6, 1974 |
|
Harvey EB, Boice JD, Honeyman M, Flannery JT: Prenatal x-ray exposure and childhood cancer in twins. N Engl J Med 312: 541, 1985 |
|
Federle MP, Cohen HA, Rosenwein MF et al: Pelvimetry by digital radiography: A low dose examination. Radiology 143: 733, 1982 |
|
Gimovski ML, Willard K, Neglio M et al: X-ray pelvimetry in a breech protocol: A comparison of digital radiography and conventional methods. Am J Obstet Gynecol 153: 887, 1985 |
|
Adam PH, Alberge AY, Castellano S et al: Pelvimetry by digital radiography. Clin Radiol 36: 327, 1985 |
|
Kopelman JN, Duff P, Karl RT et al: Computed tomographic pelvimetry in the evaluation of breech presentation. Obstet Gynecol 68: 455, 1986 |
|
Lenke RR, Shuman WP: Computed tomographic pelvimetry. J Reprod Med 31: 958, 1986 |
|
Christian SS, Brady K, Read JA, Kopelman JN: Vaginal breech delivery: A five year prospective evaluation of a protocol using computed tomographic pelvimetry. Am J Obstet Gynecol 163: 848, 1990 |
|
Gimovski ML, O'Grady JP, Morris B: Assessment of computed tomographic pelvimetry within a selective breech presentation management protocol. J Reprod Med 39: 489, 1994 |
|
Stark DD, McCarthy SM, Filly RA et al: Pelvimetry by magnetic resonance imaging. AJR 144: 947, 1985 |
|
Beers GJ: Biological effects of weak electromagnetic fields from 0 Hz to 200 MHz: A survey of the literature with special emphasis on possible magnetic resonance effects. Magn Reson Imaging 7: 309, 1989 |
|
van Loon AJ, Mantingh A, Thijn CJP, Mooyaart EL: Pelvimetry by magnetic resonance imaging in breech presentation. Am J Obstet Gynecol 163: 1256, 1990 |